Published 18 Dec 2024
Article by
4 min read
What is a SOAP Note?
A Subjective, Objective, Assessment, Plan (SOAP) note is a documentation method used by medical practitioners—such as doctors, nurses, pharmacists, and other healthcare practitioners—to assess a patient’s condition. Clinical SOAP notes are designed to improve the quality and continuity of patient care by enhancing communication between practitioners and assisting with recall of specific details.
Why Use SOAP Note Templates?
SOAP note templates are invaluable tools for standardized and efficient documentation. They provide a clear framework—Subjective, Objective, Assessment, and Plan—that ensures consistency and minimizes confusion when recording client or patient information. Following this structured format allows practitioners to save time and focus on capturing essential details rather than formatting their notes from scratch.
This approach also enhances accuracy by prompting users to include all critical data, reducing the likelihood of omissions. SOAP templates promote better collaboration by offering a language that all team members and stakeholders can easily understand. Additionally, they help ensure compliance with legal and professional standards, protecting both the provider and the client.
How to Write a Clinical SOAP Note (with Examples)
Writing in a SOAP note format allows healthcare practitioners from various fields (e.g., occupational therapy) to conduct clear and concise documentation of patient information. This method of documentation helps the involved practitioner get a better overview and understanding of the patient’s concerns and needs.
Below are SOAP note examples and walkthroughs of how you can effectively and quickly write a SOAP note following the SOAP note outline depending on your needs:
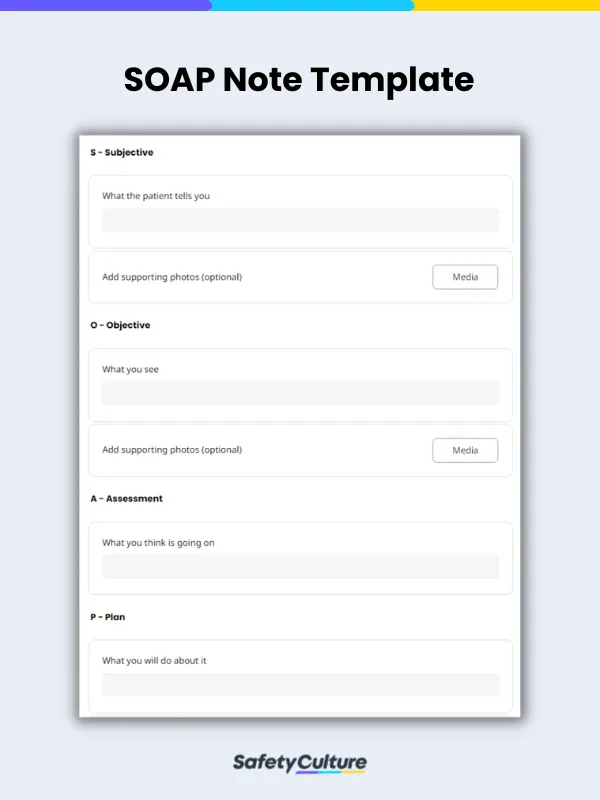
Subjective
What the Patient Tells you
This section refers to information verbally expressed by the patient. Take note of the patient ’s complete statement and enclose it in quotes. Recording patient history such as medical history, surgical history, and social history should also be indicated as it can be helpful in determining or narrowing down the possible causes.
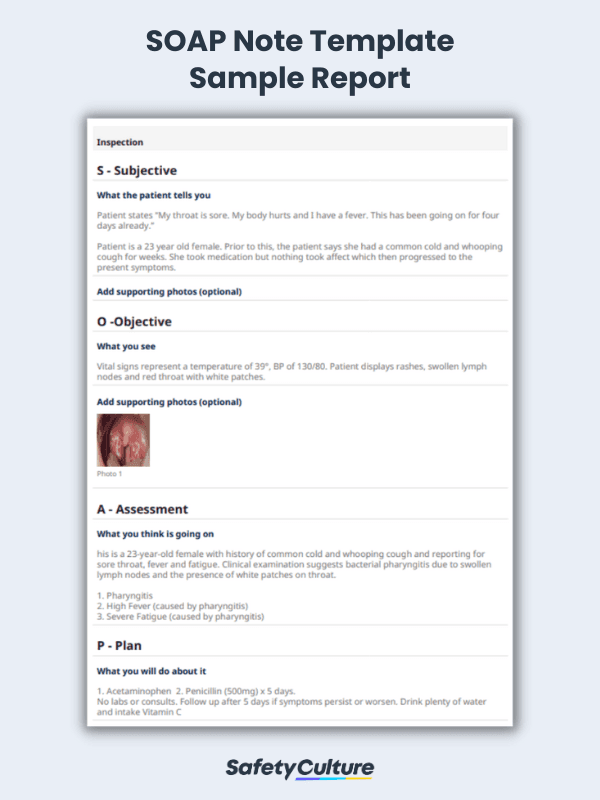
SOAP Note Example: Subjective: Patient states: “My throat is sore. My body hurts and I have a fever. This has been going on for 4 days already.” Patient is a 23-year-old female. Prior to this, patient says she had a common cold and whooping cough then progressed to the current symptoms. |
Objective
What You See
This section consists of observations made by the clinician. Do a physical observation of the patient’s general appearance and also take account of the vital signs (i.e temperature, blood pressure etc). If special tests were conducted, the results should be indicated in this section. Using the previous example, we can write the objective like this:
SOAP Note Example: Objective: Vital signs represent a temperature of 39°, BP of 130/80. Patient displays rashes, swollen lymph nodes and red throat with white patches. |
Assessment
What You Think is Going on
This section tells the diagnosis or what condition the patient has. The assessment is based on the findings indicated in the subjective and objective section. This section can also include diagnostic tests ordered (i.e x-rays, blood work) and referral to other specialists. Using the same example, the assessment would look like this:
SOAP Note Example: Assessment: This is a 23-year-old female with a history of common cold and whooping cough and reporting for a sore throat, fever, and fatigue. Clinical examination suggests bacterial pharyngitis due to swollen lymph nodes and the presence of white patches on the throat. Pharyngitis High Fever (caused by pharyngitis) Fatigue |
Plan
What You Will Do About It
This section addresses the patient’s problem identified in the assessment section. Elaborate on the treatment plan by indicating medication, therapies, and surgeries needed. This section can also include patient education such as lifestyle changes (i.e food restrictions, no extreme sports etc). Additional tests and follow up consultations can also be indicated. With the same example, the plan section can be written like this:
SOAP Note Example: Plan: Acetaminophen – take every 6 hours x 5 days Penicillin (500mg) – once a day for 5 days No labs or consults. Follow up after 5 days if symptoms persist or worsen. Drink plenty of water and intake Vitamin C |
SOAP Note Example
After the form is completed, a SOAP Note report can be generated which includes the input details of the patient. This report can be securely stored in the cloud or shared with relevant recipients in various formats. This sample report below provides a general overview of how a SOAP note report can look like, following the correct SOAP notes outline:
Still looking for a checklist?
Search, filter, and customize 60,000+ templates across industries and use cases.