Fall Risk Assessment Frequency
Generally, a fall risk assessment should be completed upon admission of the patient to effectively prevent falls or reduce the risk of falling. Apart from the initial assessment, fall risk assessments should also be completed immediately after a fall, when there is a change in the patient’s condition or medication, and before each shift for high-risk patients. Through early risk identification and reassessments, appropriate preventive measures can be in place.
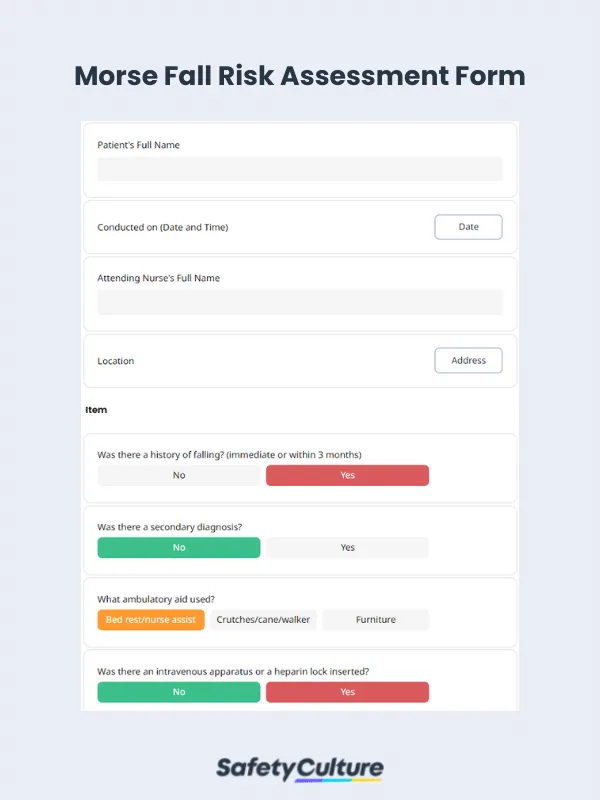
What to Include in a Fall Risk Assessment Checklist?
A comprehensive fall risk assessment checklist should cover several key items to properly identify factors that may cause an accident. Here are the essential elements to include:
History of Falls
Any falls in the past year? How many?
Injury: Were you injured in a fall?
Circumstances: What caused or triggered the fall?
Balance, Gait, and Mobility
Unsteadiness: Feel unsteady when standing or walking?
Walking aid: Use a cane, walker, or other device?
Weakness: Trouble standing up from a chair or stepping onto curbs?
Test results: Timed Up and Go, Chair Stand, or Balance Test results (if available).
Physical and Sensory Factors
Dizziness: Light-headedness or dizziness, especially when standing?
Low blood pressure: Postural hypotension (drop in blood pressure when standing)?
Foot pain or poor footwear: Foot pain lasting a day or more, or inappropriate shoes?
Environmental Hazards
Workplace safety: Loose rugs, poor lighting, clutter, or slippery floors?
Are safety signages and safety practices being followed?
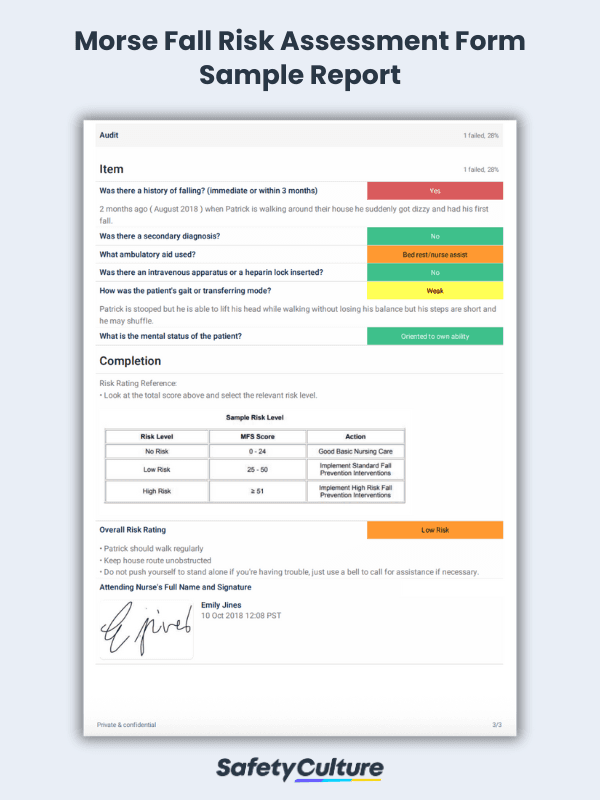
Morse Fall Risk Assessment Form Sample Report | SafetyCulture
Fall Risk Assessment Process
Derived from the fall risk assessment tool developed by Johns Hopkins, listed below are the 5 key steps of the falls risk assessment process:
Step 1: Be aware of the patient’s medical history
Having a clear understanding of the patient’s medical history, especially in areas most critical to fall risks, can help nursing personnel to carry out a fall risk assessment correctly. Knowing if the patient has a history of falls, recurrent falls, and took diuretics or narcotics, among others, can greatly inform a fall assessment, leading to a more accurate risk rating.
Step 2: Identify high or low fall risks based on certain conditions
The process of coming up with a fall risk score can be foregone when a patient is immediately identified either as a high fall-risk or a low fall-risk. A patient is automatically considered a high fall-risk if he/she has a history of more than one fall within 6 months before admission, has experienced a fall during a hospitalization period, and is deemed high fall-risk per organizational protocol (e.g. seizure precautions).
On the other hand, a patient is considered a low fall-risk when he/she is completely immobilized or in a state of complete paralysis. Either way, interventions per protocol should be implemented accordingly.
Step 3: Determine fall risk ratings based on common risk factors
When the aforementioned conditions are non-existent, the assessor should continue in the process of determining a fall risk rating by evaluating common fall risk factors such as age, medication, patient care equipment, mobility, and cognition. Assigning fall risk ratings generally follows the principle of direct correlation—the more points are earned from each risk factor, the higher that patient’s risk of falls.
Step 4: Implement risk interventions per protocol
Risk interventions vary depending on the protocols set by the healthcare institution. Sample interventions for high fall-risks include close supervision of the patient with attempts to address the patient’s risk factors and appropriate post-fall care with injury prevention measures in the case of recurrence, while the most basic risk intervention for low-risk patients is improving environmental safety, or practicing universal fall precautions such as:
Familiarize the patient with the environment.
Keep the patient’s personal possessions within patient safe reach.
Have sturdy handrails in patient bathrooms, stairs, room, and hallway.
Keep hospital bed brakes locked.
Keep wheelchair wheel locks in a “locked” position when stationary.
Keep non-slip, comfortable, well-fitting footwear on the patient.
Keep floor surfaces clean and dry. Clean up all spills promptly.
Keep patient care areas uncluttered.
Follow safe patient handling practices.
Step 5: Update patient records and reassess fall risks as required
Monitor the effectiveness of fall preventive measures applied according to a patient’s fall risk, notify all key healthcare staff, and document changes accordingly. Keeping patient records up-to-date is crucial to successfully carry out a fall prevention plan aligned with the individualized care plan.